Advances in pain treatment can be broken down into two distinct areas: pharmacological advances and procedural-based innovations. Both areas are critical to improving patient outcomes and quality of life.
I. Advances in Pharmocological Treatment
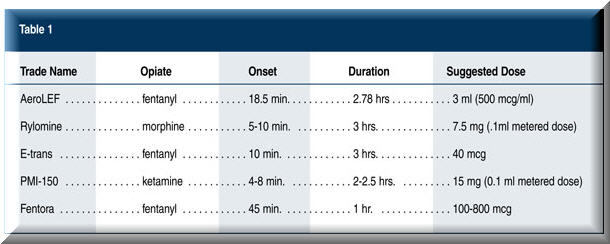
There are several new advances in the pharmacological treatment of pain that utilize novel delivery mechanisms for pain medications. At the ASA 2006 Annual Meeting in Chicago last October, several new or upcoming additions to our armamentarium were introduced, including:
• An inhaled liposome-encapsulated fentanyl preparation (AeroLEF);
• A new oral transmucosal fentanyl tablet (Fentora);
• A transmucosal patient-activated bolus of fentanyl (E-trans);
• Intranasal morphine (Rylomine); and
• Intranasal ketamine (PMI-150).
AeroLEF is an investigational fentanyl product that is delivered via an inhaled nebulized treatment. It is indicated for moderate to severe pain. The inhaled liposome-encapsulated fentanyl provides rapid analgesia and extended duration of analgesia whereby the lung serves as a reservoir for prolonged effect. Though this drug is in the initial phase of clinical studies in Canada, clinical trials are planned for the United States in the very near future. It affords patients the ability to self-titrate their analgesia. This mode of delivery may be of use in terminally ill patients for whom potent analgesics need to be administered or in patients who cannot use the oral route of administration.
Rylomine is an intranasal delivery system for morphine that is intended to target a niche portion of the opiate market where rapid onset of analgesia is needed without the need for intravenous access. It provides faster onset of action than oral morphine products, and since it bypasses the gastrointestinal (GI) system, it is associated with fewer GI side effects.
The E-trans fentanyl system is an on-demand delivery mechanism that allows patients to deliver fixed bolus doses of fentanyl of 40 micrograms each through the skin. It utilizes a low-intensity direct current to move fentanyl from a hrogel reservoir into the skin, which has been shown to be as effective as intravenous-PCA morphine. It does not incorporate a continuous infusion.
Intranasal ketamine is an NMDA receptor antagonist indicated for acute moderate to severe pain. The doses required to treat pain are 1/10th to 1/16th of those used for general anesthesia. This is currently in clinical development. Off-label use and previous studies have suggested ketamine is an effective analgesic. Its initial market will be breakthrough pain in orthopedic injuries and postoperative pain where immediate-release opioids are desirable.
Fentora is a fentanyl buccal tablet that is partially absorbed through the mouth and partly absorbed through the stomach. It has incremental doses from 100 micrograms to 800 micrograms. It is intended for breakthrough pain in cancer patients similar to fentanyl lozenges (Actiq).
These novel compounds will offer further options in the care of our patients.
II. Procedural-Based Innovations
The use of interventional procedures can be instrumental in improving outcomes for those suffering from chronic pain. In the past few years, pain physicians have been given many new tools to use in the battle against pain. New advances are important, and physicians should be aware of these issues when seeing these patients in their office. Particular areas of interest include:
• Spinal cord stimulation;
• Intrathecal drug delivery;
• Minimally invasive disc procedures; and
• Laser-guided fluoroscopy.
Spinal cord stimulation received initial Food and Drug Administration (FDA) approval in the late 1960s. For several decades, the devices consisted of simple anode and cathode arrays that delivered energy at a constant voltage with minimal choice in lead array. Over the past two years, innovations have occurred in several areas of computer technology. These advances include new leads that create a multitude of possibilities for stimulating nerves. The most advanced area of programming includes a new tripole system that focuses cathode energy to the center of the spinal cord. Other exciting areas include rechargeable batteries, independent electrode programming and constant current systems.
Intrathecal drug delivery has been used clinically for more that two decades. The advances in recent years have consisted of smaller pumps with equal or larger volumes, improvements in software programming and new research into more durable catheters by several manufacturers. The biggest advance during the last 24 months has been the approval by the FDA of ziconotide for intrathecal use. This drug, which is derived from a snail toxin, works at the calcium channels to improve neuropathic pain. This is the first drug to receive FDA approval for intrathecal use in more than a decade.
Minimally invasive disc procedures have been a focus of extensive research over the past few years. Advances include new heating probes to treat the annulus, new methods of mechanically removing the nucleus and cutting-edge laser-based techniques to treat complex disc, bone and nerve disorders. These advances may lead to a reduction in the need for costly and risky open surgical techniques.
New technology has allowed for the placement of needles and other tools under fluoroscopic imagery guided by lasers. These new fluoroscopic machines allow for a laser to show the angle of the beam both on the skin and on the X-ray. This technology makes procedures much more efficient, allows for immediate angle correction and may improve safety.
New advances in the treatment of pain will continue over the coming years. It is the responsibility of those practicing medicine to stay abreast of these developments by reading peer-reviewed journals, attending continuing medical education-accredited meetings and sharing information with their colleagues. ASA will strive to be a critical part of this advancement and exchange of information.
Timothy R. Lubenow, M.D., is Professor of Anesthesiology, Rush Medical College, and Director, Section of Pain Medicine, Rush University Medical Center, Chicago, Illinois.
Vice President
International Research Foundation for RSD / CRPS
Timothy R. Deer, M.D., is President and CEO, The Center for Pain Relief, Charleston, West Virginia.