The above algorithms are for surgery for CRPS patients. These treatment protocols are intended to minimize the risk of exacerbating CRPS. The protocols suffice for minor surgical procedures. For major surgeries, more aggressive / invasive interventions may be required. However, the risks and expense of more invasive procedures need to be weighed in relation to the potential benefits on a case-specific basis.
Example:
Major surgery on an upper or lower extremity (e.g., revision rotator cuff surgery, shoulder or hip replacement):
1. Place cervical epidural catheter immediately preoperatvely under fluoroscopy to produce unilateral epidural block
2. General anesthetic or regional anesthetic at the anesthesiologist's and surgeon's discretion. Low dose ketamine infusion is recommended (1/2 mg / kg / h)
3. Restart acetaminophen, gabapentin and celecoxib as soon as possible
4.Continuous epidural infusion of a clonidine-bupivacaine-fentanyl infusion for 5 days to 6 weeks to facilitate early physical therapy. For catheter infusions longer than 5 days, a tunneled catheter is recommended
5. Weekly evaluations by the pain medicine specialist to monitor the effects of the infusion both in terms of pain relief and side effects
6. If a longer infusion period is used the patient will need to be weaned off the clonidine and fentanyl to avoid withdrawal syndrome with PO clonidine and hydrocodone or transdermal preparations of clonidine and fentanyl
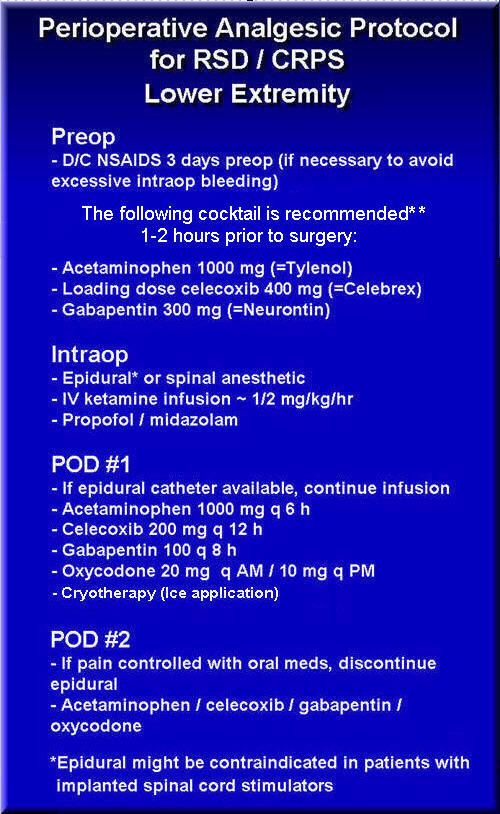
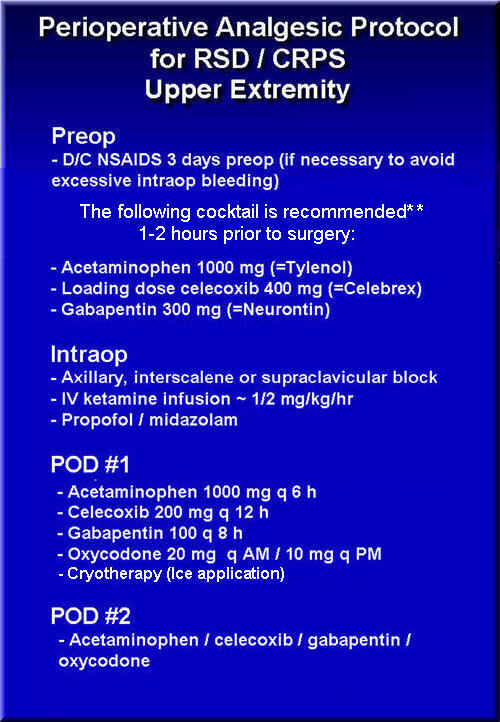
Acetominophen, celecoxib and gabapentin should be started with a sip of water just prior to surgery. However, if NSAIDs are discontinued three days prior to surgery to decrease intraoperative bleeding, these three pain medications should be started three days prior to surgery to avoid breakthrough pain.
Early ambulation and mobilization of the affected extremity is essential to the optimal rehabilitation of the patient. The cornerstone in the treatment of RSD / CRPS is normal use of the affected part as much as possible.