RSD-CRPS Physicians,
Patients Have New Internet Resource | 10-year-old boy sprains his left ankle playing baseball.He toughs out the rest of the game, but afterward he tells his mother that it hurts. Because her two older sons have sprained their ankles what seems like a million times before, she tells him to keep ice on it and rest.
A week later, the boy’s ankle still bothers him and has turned blue.Thinking a bone may be broken, the mother takes him to the emergency room for X-rays. After a long wait, the results finally come back negative for a break.The boy goes home with directions to stay off the ankle and keep icing it.
Within a matter of weeks, his entire left leg has turned blue and cold, and he can no longer put any weight on it. No doctor can explain the strange phenomenon causing him so much pain. Some go so far as to say amputation might be in order. Luckily, on their fourth specialist visit, the mother and son find out he is suffering from reflex sympathetic dystrophy (RSD), also known as complex regional pain syndrome (CRPS). The Web site for the International Research Foundation (IRF) for RSD/CRPS, www.rsdfoundation.org, provides good general information about this crippling disease. Web Site Overview The Web site offers a substantive general background on RSD/CRPS, a painful neurological disease characterized by severe burning pain, pathological changes in bone and skin, excessive sweating, tissue swelling and extreme sensitivity to
touch.
The cause of RSD remains unknown, but Anthony F. Kirkpatrick, MD, PhD, who chairs the IRF Scientific Advisory Committee, says RSD stems from the sympathetic nervous system’s normal activation following injury.
To put the process in the simplest of terms:The sympathetic nervous system ordinarily shuts down within minutes or hours after an injury; when RSD sets in,however, the sympathetic nervous system
does not shut down and begins functioning abnormally.
According to Dr.Kirkpatrick, the sympathetic outflow appears to cause pain by directly stimulating receptors on pain fibers.These events are believed to produce more pain, leading to more stimulation
of the sympathetic nervous system, which triggers another response and establishes a cycle of pain. | Thus, changes directly attributable to the abnormal sympathetic nervous system function may occur and subside over time, including changes in skin temperature and/or color, changes in sweating patterns, piloerection and swelling.
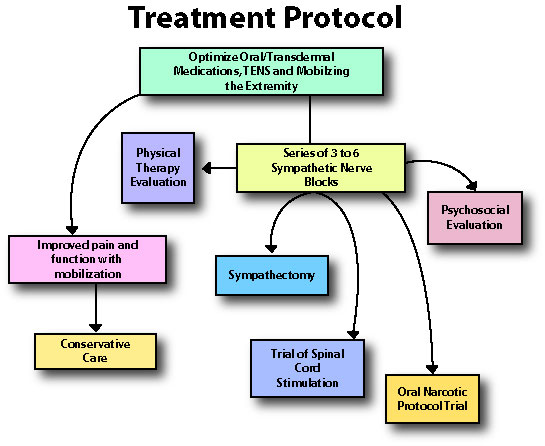
The Web site also discusses available RSD treatments. In every case, treatment should begin with patient education.The site also advises clinicians to minimize patient pain as much as possible, while encouraging patients to use their limb normally through physical therapy. If mobilization proves futile, the next step in treatment—sympathetic blocks—may be necessary.
Sympathetic blocks work through the injection of local anesthetics (e.g., lidocaine, bupivacaine) near sympathetic nerves to temporarily reverse the abnormal function and relieve the patient’s pain.
According to Dr. Kirkpatrick, the best way to conduct sympathetic blocks is in sets of three (one to two weeks apart). If, after six sympathetic blocks, the pain improves, but only temporarity, then a sympathectomy may be the treatment of choice. See Figure for a graphic representation of the treatment cycle. Web Site Layout The site offers a user-friendly, easy-to-navigate introductory page that has four language options: English, Spanish, German and French. Once you are in the language section of your choice, information is available in either video (in both downloadable
and streaming format) or transcript form. Both forms
have four sections: a message from the foundation’s president, a section on RSD’s effects on children, highlights of a panel discussion on the emotional consequences of the disease and how visitors can help the foundation. | In a web video, Dr. Kirkpatrick, founder of rsdfoundation.org, demonstrates various sympathetic nerve blocks. | | |
Page 2
| Other sections, which are more pertinent for medical professionals, are only available in text.They include more detailed medical research on treatment effectiveness, the third edition of clinical practice guidelines and research updates.
You’ll also find listings of the Board of Directors and the Scientific Advisory Committee, as well as the foundation’s mission statement and contact information. Web Site Focus Although the Web site does examine the challenges doctors may face when dealing with children afflicted with RSD, its strengths lie elsewhere. According to
P.Sebastian Thomas,MD,Professor of Anesthesiology
and Director of Pain Treatment Services, State University of New York Health Science Center at Syracuse College of Medicine, Syracuse, N.Y., “The majority of the Web site is geared toward patients or laypeople who are interested to know more about
the syndrome and how they interact with this disease:their disability,their pain and the emotional aspects of the disease.”
Robert B. Steinberg, PhD,MD, Chief of Pain Management Services, Baystate Medical Center, Springfield, Mass., agreed with Dr. Thomas, but thought that even though the Web site has a wealth of information for laypeople, it could be useful for
physicians as well.
Dr. Kirkpatrick says that, according to recent research, it is essential that both physicians and patients alike understand the clinical information.“One of the major reasons why physicians do not follow clinical practice guidelines is that most are not concise enough for both physicians and patients to read, understand and follow,” he said. “I think the section on diagnosis is pretty good,” Dr. Steinberg
says.“The most important thing for non–pain physicians to know is to make the appropriate referral early in the course of the syndrome. For primary care doctors, this kind of resource is quite important, because you can avoid the irreversible end stages.” Perhaps the most powerful area of the site is that dedicated to a panel of four children who either suffer from RSD or have beaten the syndrome after undergoing their treatment progression. | One girl was cured after three sympathetic blocks, combined with psychological and physical therapy. Another girl had to undergo the same, plus a sympathectomy, to find relief. | | In a web site video, 15-year old Amanda Alberigi discusses how a sympathectomy cured her of RSD of the right upper extremity. | Seeing and hearing the troubles these young people have gone through provides a way for doctors to appreciate the plight of children dealing with RSD.“It gives a good patient perspective,” Dr. Thomas said.“They are describing what we [doctors] do and the emotional conditions they go through. The section on pediatrics is well done. It has nice interviews with
the children—I like that part.”
The diagnosis should be established as soon as possible since treatment is thought to be most effective early in the disease process.
According to Dr. Kirkpatrick, doctors have yet to put a specific clock on how early you must catch the disease to cure it because it is a fluid condition that changes from patient to patient.Dr.Kirkpatrick has cured some war veterans who have been afflicted with RSD for upward of 50 years, but conversely has not been able to cure individuals who have suffered for only one or two years.
“Overall, I’d give it an A–,” Dr. Steinberg says. “Its most compelling strength is that there’s not anything else close to this Web site in terms of quality and comprehensiveness.” —Blaine Dionne
Based on interviews with Anthony F. Kirkpatrick, MD, PhD, P. Sebastian Thomas, MD, and Robert B. Steinberg, MD, PhD. | The International Research Foundation for RSD/CRPS is a 501(c)(3) (not-for-profit) organization in the United States of America.
HOME | MENU | DONATE | CONTACT US
Reflex Sympathetic Dystrophy (RSD) | Complex Regional Pain Syndrome (CRPS)
Copyright © 2003 International Research Foundation for RSD/CRPS.
All rights reserved.
For permission to reprint any information on the website, please contact the Foundation.
|