[Case Reports with Video]
Cantu, Fernando M.D.*, Hoffman, Richard Ph.D.†, Schwartzman, Robert M.D. §, Kirkpatrick, Anthony M.D., Ph.D‡
*Staff Anesthesiologist, San José Hospital, Technological of Monterrey, School of Medicine, Monterrey, México, †President, International Research Foundation for RSD / CRPS, Tampa, Florida, §Professor, Department of Neurology, Drexel University College of Medicine, Philadelphia, Pennsylvania, ‡Chairman, Scientific Advisory Committee, International Research Foundation for RSD / CRPS, Tampa, Florida
Support provided by the International Research Foundation for RSD / CRPS.
Address correspondence to Dr. Kirkpatrick: International Research Foundation for RSD / CRPS, 7612 Woodbridge Boulevard, Tampa, Florida 33615
Click HERE for video web enhancement for Case 1
Click HERE for video web enhancement for Case 2
Advanced complex regional pain syndrome (CRPS) remains difficult to treat. Low dose ketamine infusions for 5 to 10 days have been studied as a possible treatment for advanced CRPS. (1) In that study there were several issues complicating the interpretation of the data, including the lack of data on outcome other than self-reporting of pain by the patient. Nonetheless, low doses of ketamine sufficient to maintain consciousness produced significant relief of pain during the infusion but the infusion also produced temporary deficits in attention, memory, and executive function.Patients typically described a feeling of inebriation, blurred vision and nausea. (1- 3)
High doses of ketamine sufficient to induce general anesthesia for 5 days have been studied in Germany. (4, 5) In this open label study, 50% of twenty patients with advanced and intractable CRPS were pain free at six months and no significant complications from either a psychiatric or medical point of view were reported. (5) These initial results are impressive and need to be replicated.
We report two cases of patients with refractory CRPS who obtained an improvement in pain and function following five days of general anesthesia with ketamine and midazolam. In case 1, multiple attempts at low dose ketamine infusions failed to produce a sustained improvement in pain and function. Only when doses of ketamine were sufficient to maintain general anesthesia for five days was it possible to obtain a long-lasting remission of pain due to allodynia. In case 2, we obtained some important information about a possible role of high dose ketamine in treating skin ulcers due to CRPS. Trophic skin ulcers are a known complication of CRPS that predispose patients to severe infections caused by streptococci and anaerobic bacteria. (6) When these bacteria are resistant to antibiotics, amputations are sometimes necessary. (7)
Both cases fulfilled the IASP diagnostic and modified research diagnostic criteria for CRPS. (8) Anesthesia was induced with intravenous ketamine (0.5-1 mg/kg) and midazolam (bolus of 2.5-6 mg). Succinylcholine (1.5 mg/kg) was used to facilitate intubation. The initial rate of ketamine and midazolam infusion was based on actual patient body weights. Two methods were used to determine the effects of high dose ketamine on pain and function. Static mechanoallodynia was measured as a component of pain. This measurement is an objective and more specific sign of pain due to CRPS than self-reporting of pain scores. (9) Pain thresholds were measured by applying pressure to the skin using an algometer force gauge. (10) Pressure was applied at a straight angle to a defined surface of the body at a speed of 1 kg/s. Research subjects were blinded to the measurements generated by the force gauge. The pain thresholds were measured as the force applied to skin that was necessary in order for the patient to report that the sensation of pressure was converted to a sensation of pain. The measurements were repeated three times at each site and the mean was accepted. Video recordings documented physical impairment before and after the ketamine-midazolam infusion. Cognitive function was measured both before and one month following the infusion using the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). (11)
The study was approved by the Institutional Review Board for San José Hospital, Technological of Monterrey, School of Medicine, Monterrey, México. After obtaining written informed consent, general anesthesia was induced.
Case Reports
Case 1
A 15-yr-old, 35-kg female presented with a 2-year history of CRPS of the lower extremities. Despite aggressive medical management which included multiple trials of antidepressants, anticonvulsants, sympathetic nerve blocks, a trial of spinal cord stimulation and physical therapy in a comprehensive pain management program for one month, the patient’s symptoms due to CRPS became progressively worse. At that point, low dose ketamine infusions were performed on three separate occasions. The infusion of administered ketamine ranged from 7 to 16 mg h -1 lasting for 5 to 10 days for each infusion. During the low dose ketamine infusions, the child experienced complete relief of her pain due to allodynia. The relief of pain was associated with profound amnesia. Unfortunately, each time the low dose infusion of ketamine was stopped, pain due to allodynia returned immediately to the pre-infusion level. During the course of low dose ketamine infusions, CRPS spread to the upper extremities.
The patient was admitted to the intensive care unit and central intravenous and arterial cannulae were inserted and electrocardiogram electrodes and pulse oximetry sensor were applied. The patient was intubated following a loading dose of ketamine and midazolam. The dose of ketamine and midazolam was adjusted over the 5-day infusion in order to maintain adequate anesthesia. (Table 1).
Table 1. Dosages of ketamine and midazolam during anesthesia in patient in Case 1.
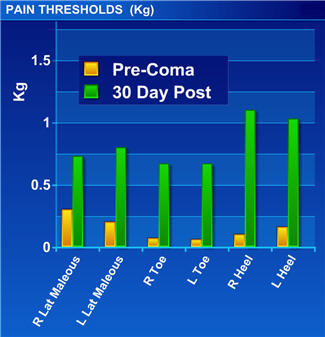
Cardiovascular parameters were stable throughout the infusion. Upon emergence from general anesthesia, the patient developed hallucinations that were controlled with propofol and midazolam. The patient was discharged from the hospital three days after extubation. One month after the ketamine procedure a significant improvement in pain thresholds was noted. (fig. 1) There was no decline in cognitive function one month following the high dose ketamine procedure based on the RBANS total score for the patient.
Fig. 1 Pain thresholds before and after the ketamine anesthesia in patient in Case 1. The measurements were repeated three times at each site and the mean was accepted.
Following the high-dose ketamine procedure, allodynia completely disappeared and the patient was able for the first time to shower, wear shoes, climb stairs, sleep with sheets, tolerate wind and rain.
Click HERE for the video web enhancement for Case 1.
Case 2
A 37 -yr-old, 47-kg physician presented with a 7-year history of CRPS that was initially in the right upper extremity but then spread to all four extremities and the face. At the time the patient presented to University of South Florida in 2007, open ulcers were rapidly spreading in the upper extremities and becoming more painful. (fig. 2). Raindrops touching the skin caused unbearable pain. Despite aggressive medical management which included opioids, anticonvulsants, antidepressants, and sympathetic nerve blocks the patient became confined to a wheelchair and unable to work.
Fig. 2. Skin ulcers before anesthesia in patient in Case 2.
The patient was admitted to the intensive care unit and central intravenous and arterial cannulae were inserted and electrocardiogram electrodes and pulse oximetry sensor were applied. The patient was intubated following a loading dose of ketamine and midazolam. The dose of ketamine and midazolam was adjusted over the 5-day infusion in order to maintain adequate anesthesia. (table 2).
Table 2. Dosages of ketamine and midazolam during anesthesia in patient in Case 2.
Discussion
Windup and central sensitization are key neurological processes that appear to be involved in the induction and maintenance of CRPS/neuropathic pain. Because over excitation of the N-methyl-D-Aspartate (NMDA) receptor complex appears to play a major role in the development of these phenomena, there have been efforts made by many over the past 20 years to treat chronic pain using NMDA antagonists. (12-16)
Ketamine was used for most of these studies, as it is the most potent clinically available NMDA-antagonist. Drugs such as dextromethorphan, amantadine, and memantine, although relatively safe (from a central nervous system side effect standpoint), have relatively weak NMDA receptor-inhibition activity and appear to have a low potential for blocking the sensitization process.
There is no control group in the current study. Therefore, we do not know if the benefits of five days of general anesthesia are unique to ketamine. Given the impressive results and the relatively high risks associated with this protocol, it might be difficult to recruit patients to a control where general anesthesia is administered for five days without ketamine.
In the first case reported here, the patient required doses of ketamine 12 to 30 times higher than those used for the low dose ketamine technique in order to achieve a long-lasting relief of pain due to allodynia. Although the low dose ketamine infusion provided temporary relief of pain during the infusion, the low-dose procedure was associated with profound amnesia, making it difficult for the patient to carry out activities of daily living. In the second case, there was healing of skin ulcers noted 2 to 3 days after the high-dose ketamine-midazolam infusion. The ulcers disappeared and the patient returned to normal activities in three months. To our knowledge, this is the first report of skin ulcers healing during a ketamine infusion.
Unlike previous studies, these case reports included more than self-reporting of pain as an assessment of response to ketamine infusion. (1, 4-5) Pain was measured by determining pain thresholds for static mechanoallodynia and functional improvement was documented utilizing serial video recordings. Our study suggests that doses of ketamine and midazolam sufficient to maintain general anesthesia for five days may be useful to treat advanced CRPS refractory to conventional treatment options. It must be emphasized that this protocol is associated with serious risks. Infectious complications still represent the main source of morbidity and mortality in modern intensive care medicine.
References
1. Correll GE, Maleki J, Gracely EJ, Muir JJ, Harbut RE. Subanesthetic ketamine infusion therapy: A retrospective analysis of a novel therapeutic approach to complex regional pain syndrome. Pain Med 2004; 5: 263-75
2. Anand A, Charney D, Berman R, Hu X, Cappiello A, Krystal J. Attentuation of neuropsychiatric effects of ketamine with lamotrigine: Support for hyperglutamatergic effects on N-methyl-D-aspartate receptor antagonists. Arch Gen Psychiatry 2000; 57: 270-76
3. Krystal H, Abi-Saab W, Perry E, DeSonza D, Liu D, Gueorguierva R, McDougall L, Hunsberger T, Belger A, Levine A, Breier A. Preliminary evidence of attenuation of the disruptive effects of the NMDA glutamate receptor antagonist, ketamine, on working memory by pretreatment with the group II metabotrophic glutamate receptor agonist, LY 354740, in healthy humans. Psychopharmacology 2005; 179: 303-9
4. Koffler SP, Hampstead BM, Irani F, Tinker J, Kiefer RT, Rohr P, Schwartzman RJ. The neurocognitive effects of 5 day anesthetic ketamine for the treatment of refractory complex regional pain syndrome. Arch Clin Neuropsychol 2007; 6: 719-29
5. Kiefer T, Rohr P, Poppa A, Dieterich H, Grothussen J, Koffler S, Altemeyer K, Unerti K, Schwartzman R. Efficacy of ketamine in anesthetic dosages for the treatment of refractory complex regional pain syndrome (CRPS)An open label phase II -study. Pain Med 2007; (in press).
6. Webster G, Schwartzman R, et. al. Reflex sympathetic dystrophy: Occurrence of inflammatory skin lesions in patients with Stage I and II disease. Arch Dermat 1991; 127: 1541-44
7. Dielissen PW, Classen AT, Veldman PH, Goris JA. Amputation for reflex sympathetic dystrophy. J Bone Joint Surg (Br] 1995: 77:270-3
8. Bruehl S, Harden RN, Galer BS, Saltz S, Bertram M, Backonja M, Gayles R, Rudin N, Bhugra MK, Stanton-Hicks M. External validation of lASP diagnostic criteria for complex regional pain syndrome and proposed research diagnostic criteria. International Association for the Study of Pain 1999; 81: 147-54.
9. Bennett D, Brookoff D. Complex Regional Pain Syndromes (Reflex Sympathetic Dystrophy and Causalgia) and Spinal Cord Stimulation. Pain Med 2006; 7:64-96
10. Algometer Pain Diagnostic Gage. Models FPK 2 and FPK 5 were used. Wagner Instruments. Greenwich, Connecticut, USA.
11. Gold JM, Queern C, Iannone VN, Buchanan RW. Repeatable Battery for the Assessment of Neuropsychological Status as a screening test in schizophrenia, I: Sensitivity, reliability, and validity. Am J Psychiatry 1999; 156:1944-1950
12. Hunt SP, Mantyh PW. The molecular dynamics of pain control. Nature Reviews 2001; 2: 83-91.
13. Woolf CJ, Salter MW. Neuronal plasticity: Increasing the gain in pain. Science 2000; 288: 1765-68
14. Schwartzman RJ. New treatments for reflex sympathetic dystrophy. N Engl J Med 2000; 343: 654-6
15. Lavand’homme P, DeKock M, Waterloos H. Intraoperative epidural analgesia combined with ketamine provides effective preventative analgesia in patients undergoing major digestive surgery. Anesthesiology 2005;103:813-20
16. Suzuki M, Haraguti S, Sugimoto K, Kikutani T, Shimata Y, Sakamoto A. Low-dose intravenous ketamine potentiates epidural analgesia after thoracotomy. Anesthesiology 2006;105:111-9
Appendix
1. Written consent from research subject to publish the video evaluations on the world wide web:
Shannon Stocker MD ... CLICK HERE
2. Electronic copy of "In Press" manuscript cited:
Kiefer T, Rohr P, Poppa A, Dieterich H, Grothussen J, Koffler S, Altemeyer K, Unerti K, Schwartzman R. Efficacy of ketamine in anesthetic dosages for the treatment of refractory complex regional pain syndrome (CRPS)An open label label phase II -study. Pain Med 2007; (in press).
... CLICK HERE