The recent introduction of rechargeable neurostimulation systems to the market represents a significant advance in treating chronic pain. To make an informed choice about neurostimulation systems, patients and their physicians should consider the pertinent differences among the conventional and rechargeable systems. . Rechargeable systems have quickly become the most frequently implanted type of spinal cord stimulating system. This publication includes access to a free video "Device Selection Criteria for SCS Systems" at the bottom of this page.
The authors plan to update this web site periodically with new developments in the field of neurostimulation.
Three Types of SCS Systems
All neurostimulation systems use low-intensity electrical impulses to keep the pain signals from reaching the brain. These electrical impulses produce a tingling or massaging sensation known as paresthesia. When patients are selected carefully and the systems’ electrodes are positioned properly, neurostimulation can be a successful therapy for certain types of neuropathic pain.
Neurostimulation systems typically consist of three components designed to work together:
Leads—Leads are very thin cables, or wires, with small electrodes that deliver the electrical impulses to the nerves
Generator—The generator is the power source that sends electrical energy to the electrodes
Patient Programmer—The programmer allows the patient to change programs and turn the stimulation up or down
Three types of neurostimulation systems are used: radio-frequency (RF), conventional implantable pulse generator (IPG), or rechargeable IPG systems.
The use of radiofrequncy systems which utilize an outside battery has decreased dramatically since the introduction of rechargeable technology. The merits of the systems are often debated, and the efficacy of each can vary from one patient to another, from one body area to another, and from one disease state to another. Additionally, research is still needed to determine whether incisions made when implanting the system can result in the spread of RSD to other parts of the body.
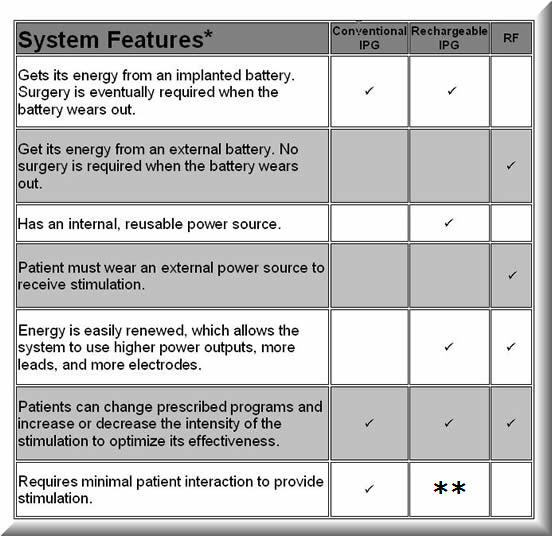
The systems have many similarities (as shown in the illustrations at the bottom of this page), but there are important distinctions between the systems that patients and clinicians should consider when choosing a system. A brief comparison of system features is given in the Table I.
TABLE I
*The designs of current RF and IPG systems vary, and these statements may not apply to all designs. Future designs may overcome these limitations and provide new options.
**Rechargeable systems require patient interaction to recharge the system, but are otherwise similar to conventional IPG systems.
RSD/CRPS is sometimes a migrating or progressive disease: pain may begin in one area or extremity, only to spread and involve other extremities. This progression can significantly increase the power and electrode requirements for RSD/CRPS patients. Patients also should be aware that, because the systems contain metal, if they receive an implanted system, they cannot be exposed to magnetic resonance imaging (MRI).
As a general rule, patients with pain in a single extremity might be the appropriate candidates for a conventional IPG. The energy requirements for their pain are low, and they would not have to use an antenna on a possibly sensitive implant site. Patients with upper extremity pain, which may involve a hand or arm that would control the implanted device, may benefit from a conventional IPG which requires less effort. On the other hand, patients with lower extremity and/or multiple extremity pain may require an RF system or a rechargeable IPG that can operate at higher power levels and disperse stimulation to multiple parts of the body.
Cost Effectiveness
A cost analysis study was conducted by Bell et al. in a population of failed back surgery patients suffering with neuropathic pain. (1) These investigators compared treatment costs for surgery and other therapies with spinal cord stimulation. The estimates of medical resource utilization were based upon diagnostic and therapeutic protocols of the North American Spine Society, protocols for spinal cord stimulation (SCS), c1inical literature, and actual data of complication rates in patients treated with SCS at Johns Hopkins University.
The model looked at costs generated annually for two groups over a five (5) year period to determine the payback period. (The payback period is the length of time before the savings due to SCS treatment are sufficient to compensate for the greater initial costs of implantation) The two groups were:
Two identical failed back surgery patients, each assumed to suffer from debilitating long-term back pain after at least one failed back surgery and currently preparing to undergo another back surgery.
The model assumed that one patient would continue to be treated and managed using a representative mix of non-SCS therapies, while the other would undergo SCS screening and subsequent implant, if appropriate.
The medical cost savings were found to pay for SCS therapy in an average of 3.2 to 5.5 years depending on the set of assumptions used in the model. For patients responding well to SCS, payback was within 2.1 years. Over a five year period, it was estimated that $27,970 would be saved with a fully implanted system, while $39,340 was saved using a radio-frequency system.
Rechargeable SCS Systems
To make an informed choice about a neurostimulation system, patients and their physicians should consider the patients' current pain patterns, the possibility of progression of the patients’ disease, and the pertinent differences between RF, conventional IPG, and rechargeable IPG systems. The relative difference in parameters offered by rechargeable IPG systems are outlined in Table II.
TABLE II
Parameter
Medtronic
"Restore"
Boston
Scientific
"Precision"
ANS
" Eon™ "
Number of Electrical Contacts
16
16
16
Vertebral Segments
Covered
2
1
2
Battery
Life
(FDA Labeling)
9 Years (power level not defined by FDA)
5 Years
Medium
Power
7 Years
High
Power
Battery
Strength
(mA)
300 mA
200 mA
325 mA
Zero-Volt
Battery
Technology
No
Yes
No
Battery
Warranty
1 Year
5 Year
1 year
Current
Delivery
Constant
Voltage for
Each Array
Constant
Current
Independent
for
Each Electrical
Contact
Constant
Current for
Each Array
Frequency
Range
Maximum -
260
Pulse/second
Hz
Maximum - 1200
Pulse/second
Hz
Maximum - 1200
Pulse/second
Hz
Multiplexed Channels per Program
Up to 4
1 set @ 130 Hz
2 sets @ 130 Hz
4 sets @ 65 Hz
Up to 4
1 set @ 1200 Hz
2 sets @ 130 Hz
4 sets @ 80 Hz
Up to 8
1 set @ 1200 Hz
2 sets @ 600 Hz
4 sets @ 300 Hz
8 sets @ 150 Hz
Maximum
Pulse Width
(Microseconds)
450
1000
500
# of Programs
1 to 32
1 to 4
1 to 24
MultiStim®
4
4
8
Current
Steering
Manual
Automatic
Manual
Compatible Percutaneous Leads
6
1
5
Compatible
Surgical Leads
4
1
10
Maximum Implantation Depth
2.5 cm
2.0 cm
2.5 cm
Size
72 gm/
39 cc
36 gm/
22 cc
75 gm/
42 cc
Magnet
Option
No
No
Yes
Recharge
Time
(After
Complete
Discharge)
6 Hours
Battery Might Not Tolerate More than 3 Complete
Drains.
*
4 Hours
4-5 hours
Charging
Mechanism
Portable Charge Available**
Portable Charge with Possible heat buildup
AC Plug
Required
*The statement “battery might not tolerate more than 3 complete drains” warrants clarification. If the battery has reached a level where recharge is required everyday, the patient will be prompted to begin recharging. Technically, if the device is over-discharged for longer than 60 days three separate times, the battery should be replaced. Medtronic writes, "If the patient is not motivated to recharge for three consecutive cycles of 60 days, there is a good chance that the therapy is not adequate and the stimulator should be explanted anyway".
**The Restore recharger by Medtronic contains a temperature sensor that will disable the recharger to ensure it stays below 41° C (a standard to ensure patient comfort and safety).
# The concern regarding the reports of heating during recharging have been addressed. The new charging mechanism has a temperature sensor which disables the recharger to ensure it stays below 41 degree C
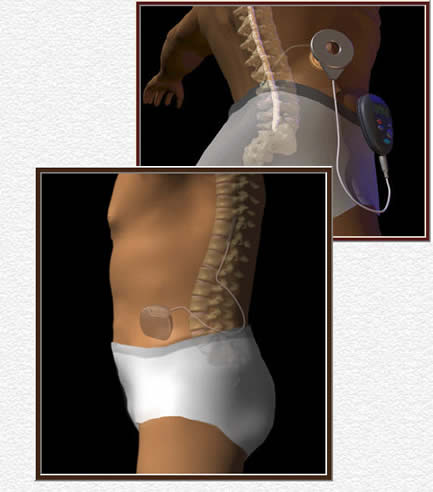
External and Internal Battery
SCS Systems
External Battery System Radio Frequency (RF) System
Internal Battery System
Implantable Pulse Generator (IPG)
(Conventional or Rechargeable)
DISCUSSION
Here are some differences among rechargeable IPG systems that are important to consider in patients with RSD / CRPS:
BATTERY STRENGTH (mA)
The greater the amp output of the battery, the greater the time between charges for a given stimulation pattern.
ZERO-VOLT TECHNOLOGY
Zero-Volt Technology uses battery chemistry: where the inactive salt byproducts formed by normal battery use don’t corrode the battery poles. This technology allows the battery the ability to recharge after being completely drained multiple times. With Zero-Volt technology, the physician need not worry about the patient forgetting to charge their IPG.
CURRENT DELIVERY
Over a period of time, it is expected that changes in impedance due to scar formation will change the current flow or electrical stimulation. This change in electrical stimulation might require that the SCS system be reprogrammed. The more the independent the constant current flow to an electrical contact, the more likely the electrical will maintain a given stimulation pattern without the need to change the program of the SCS system. The Advanced Bionics rechargeable SCS system is the only SCS that provides constant current to each individual electrical contact. The ANS rechargeable SCS system provides constant current flow to an array of electrical contacts along a lead. In vivo clinical studies are needed to determine the relative magnitude of the presumed benefits of the different types constant current systems for SCS.
FREQUENCY:
The higher the frequency, the greater the potential therapeutic efficacy in patients with RSD / CRPS, especially in managing breakthrough pain. (2,3)
However, because high frequency stimulation demands increased energy consumption, high frequency stimulation requires increased daily/weekly recharge sessions.
MultiStim®
MultiStim® consists of stimulating alternatively more than one region of the body. MultiStim® may be of special benefit when there is more than one site to stimulate and where higher frequencies are required, as is often the case in patients with RSD / CRPS. The rechargeable ANS system appears to provide the higher frequencies when used in the MultiStim® mode. To determine the frequency during Mutistim for the various rechargeable SCS systems, see “Multiplex Channels per Program” in Table II above.
CURRENT STEERING
The automatic steering seems to facilitate more efficient programming because the patient, rather than the health provider, manipulates the controls for programming. In addition, the patient benefits by having a greater sense of control of their pain. However, the patient needs to come to the physician’s office to use the programmer (which costs approximately $5,000 per unit). The long-term outcome automatic steering compared to manual steering in finalizing electrode placement will be determined by future clinical studies. (4,5)
PULSE WIDTH
Ability to control pulse width dictates nerve fiber recruitment. Looking at a strength duration curve shows that smaller nerve fibers have higher triggering thresholds. By increasing pulse width, the duration of stimulation increases taking more nerves to threshold. Theoretically this added recruitment helps with capturing and maintaining low back coverage.
MAXIMUM IMPLANTATION DEPTH
A greater implantation depth gives the surgeon more freedom in selecting a site for implantation. In addition, a greater implantation depth guards the patient from the adverse effects of weight gain in the future.
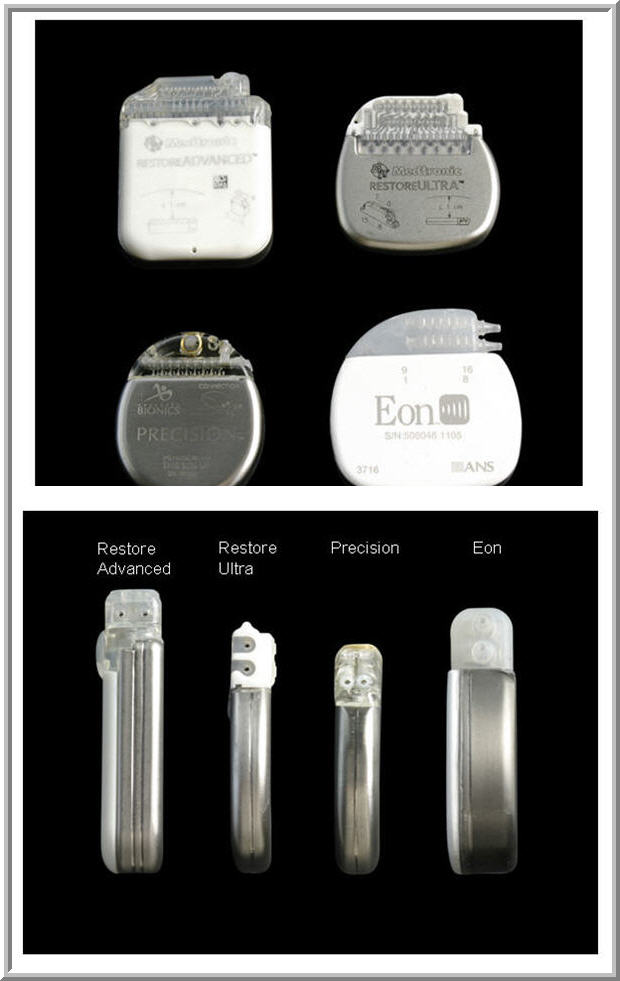
SIZE
The image below illustrates the relative size of the three rechargeable SCS devices
1. Bell G, Kidd D, and North R. Cost-Effectiveness Analysis of Spinal Cord Stimulation in Treatment of Failed Back Surgery Syndrome. J Pain Symptom Manage 1997; 13: 286-295.
2. Kemler MA, Barendse GA, et al. Spinal cord stimulation in patients with chronic reflex sympathetic dystrophy. N Engl J Med 2000;343:618-24
3. Bennett DS, Alo KM, et al. Spinal cord stimulation for complex regional pain syndrome I: a retrospective multicenter experience from 1995 to 1998 of 101 patients. Neuromodulation 1999; 2:202-210
4. Oakley J, Varga C. et al. Real-time parathesia steering using continuous electrical field adjustment . Part I: Intraoperative performance. Neuromodulation 2004; 3:157-167